


How to Make Your 80s Miserable
Breaking the news about osteopenia

Trudy* had a med check appointment for her high blood pressure, but before I could even look at the numbers, she blurted out,
When the nurse called me to tell me about my bone test results, she said I had something I’d never heard of and that I should take calcium and I hate taking calcium because it makes me so constipated and she couldn’t really tell me what to do and I wanted to talk to you about it.
Hopefully her blood pressure is ok, because I can see what we’ll be talking about today.
I’m sorry that was so confusing! Let me remind myself what your bone density test results say.
I open up Trudy’s chart. While doing so I recall Trudy and her lively household. She makes dinner for all seven of her grandchildren once a month and insists that they all come over. She started this when they were in grade school, when it was a privilege of starting first grade to be included at the cousins’ dinner. Now that they had aged into high school, they continued coming faithfully.
To be honest, I was always a little envious of those grandchildren for having a grandmother who could build that kind of structure for them.
However, remembering the details of diagnostic studies that Trudy had two months ago was not as fun or as easy as imagining the details of the cousins’ dinner. I maneuvered my cursor and pulled up the test results.
Trudy had had a bone density study two months ago. It was her second. The first, when she turned 65, had been normal. This one, ten years later, showed a decline in bone strength at all sites measured.
I explained the results to Trudy,
OK. Your bone density showed you have osteopenia. That means that your bones are not of normal strength, but they are not so fragile as to be called osteoporosis. It’s a warning to do what we can to shore up your bones. Last time your bone density was normal and this time it’s worse so whatever you have been doing for your bones is not working well enough.
Trudy replied,
Well, I’m not doing much, but this doesn’t really make sense! Almost all my friends have osteoporosis anyway, so I wonder if I need to really worry about it. I think it might be a natural part of aging. I can’t take calcium. The pills make me choke and if I get it down, it makes me constipated. Constipation is one thing I can’t stand.
My friend, Sally, her dog knocked her over, and she broke her hip and she ended up in the hospital. She had to go to rehab at a nursing home afterwards. No, thank you! I don’t want that to happen to me. That was from osteoporosis, right? Her doctor said she had to take a shot.
Osteopenia is a warning
I nodded and smiled at Trudy to let her know I’d heard her and was getting ready to respond. The points I wanted to communicate were:
Osteopenia is halfway between normal and osteoporosis.
It might be fair to say Osteoporosis is normal for postmenopausal women, because it certainly is common. But common doesn't mean that it’s okay. Osteoporosis puts patients at risk of debilitating injuries. It needs to be treated.
An osteoporotic fracture would be bad for her quality of life. Avoiding hip, wrist, and back fractures after minor accidents, like the fall her friend experienced, is the whole point of addressing osteopenia.
Osteoporosis can lead to misery, especially when it degrades the spine.
She should try to figure out how to get more calcium.
There are other things she should be doing besides taking calcium and vitamin D. It sounds like she’s not doing those things.
I think patients do better if they have a scaffolding to attach all the details I need to tell them. It’s almost always best to start by reminding them why they care about the thing we’re going to talk about and then giving them the medical explanation of what normal is, and what has gone wrong for them at whatever level I think the patient can understand given their attention span, level of pain, curiosity, etc.
I use the story about Trudy’s friend to launch my lecture.
Yes, I’ve had two patients who got tangled up in their dog’s leash and one who got jumped on and knocked over. They all broke their hips due to osteoporosis. Even tripping over a rug and falling can be enough to break a hip or a wrist if your bones are fragile enough.
The worst fractures are in people’s backs, though. You know how some women have that hump in their back – it’s called kyphosis. They get that way from lots of little fractures in their back from osteoporosis. And you know how some women lose inches of height? Osteoporosis.
Adult onset scoliosis? In my experience, it is usually part of the same process. And the worst is when women lose so much height that they end up with the bottom of their rib cages resting on their hip bones. Then they start having pain from the bones that are not supposed to be touching clacking against each other. On top of that they can’t breathe very well.
Trudy has been listening and nodding. I know she has seen every one of these situations among her friends and family.
Bones are dynamic structures
Humans’ bones are constantly keeping in balance between bone formation and bone destruction. When you hit your arm hard, for example, hard enough to think “I’m glad I didn’t break it!” you might cause some little hairline cracks that don’t go very far into the bone.
In situations like this, your body sends out some cells that chew up the damaged parts of the bone and then another kind of cells come in and replace the removed parts of bone so that the cracks all disappear. The result is the bone is all fixed (usually).
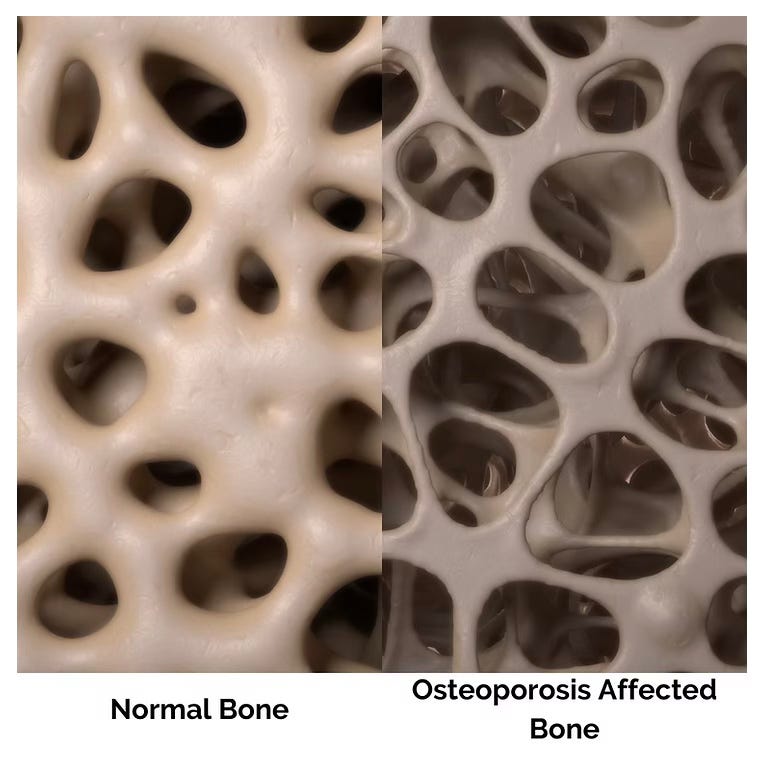
When women go through menopause, the cells that break down bone go crazy. They start chewing up perfectly fine bone so quickly that the cells that create replacement bone cannot keep up. We don’t know why this happens, but in just a few years it can turn good bone tissue into something that looks like a cheap, holey sponge.
If you start with good strong bone tissue, you can lose some and not be in danger, but if you start with bones that are already on the smaller side or if your bone-eater cells go super crazy, you can end up with bones that are prone to breaking with just a minor injury, like falling from a standing position on the ice.
There are factors other than menopause that increase the likelihood of osteoporosis (alcohol consumption, tobacco use, small stature, low BMI, family history of osteoporosis, European ancestry, low calcium intake, high calcium excretion).
Consequently, men and premenopausal women can get osteoporosis, too. Also, the situation is usually worse for women who experience premature menopause.
There are things you can do to prevent osteoporosis
The easiest way to prevent osteoporosis is to put minor stresses on your bones frequently through weight-bearing exercises.
To make sure your body has all the raw materials it needs to make bones you need calcium and vitamin D. The recommendation for calcium for post-menopausal women is 600mg two times daily. As Trudy has pointed out, calcium is constipating. An article about constipation is in the pipeline, but it is taking me a while to get it out.
I am unaware of any form of calcium that is less constipating, but there are many forms of calcium that are more pleasant to take than the huge tablets sold in stores.
You can get smaller tablets. You just have to take more of them.
Calcium comes in a chewable form (with sugar and chocolate, malt, or caramel flavoring added).
Dairy products are a great source of calcium. 1 cup of milk has 300mg of calcium in it. A grande latte at Starbucks contains 1.8 cups of milk, (540mg of calcium). Dunkins is not so forthcoming about how much milk is in their latte, but you can probably give it a good guess.
Search online to learn about other dietary sources of calcium. Many kinds of foods are good sources of calcium.
If you have other medical problems or issues with certain foods, talk with your doctor for recommendations that are best suited for you.
If you have had kidney stones it is especially important to do this. You may need more than just a consultation with your doctor. You may need to see a specialist in calcium metabolism.
We don’t have a standard recommendation on how much vitamin D you should take. Some people don’t need a supplement. Others need different levels of supplementation. Commonly 800 IU/day is suggested. However, when I test vitamin D levels in my patients I find that 800 IU is not enough. I therefore usually suggest 2,000 IU daily.
Some versions of Medicare will pay for a vitamin D test with the diagnosis of osteoporosis and some will not. All Medicare products will pay for checking vitamin D if a woman has a diagnosis of vitamin D deficiency. The safest bet is to get your vitamin D level checked when you are not taking a supplement and when you are not on Medicare. Then the diagnosis of vitamin D deficiency can be established. With that, Medicare will pay for rechecking your vitamin D levels going forward. Talk to your doctor about your situation.
Unlike vitamin D, usually it’s unnecessary to check the levels of calcium in the blood. The body carefully regulates the calcium level in the blood. If there isn’t enough, it will pull calcium from the bones to maintain the blood level. If there’s too much, it will just be excreted in the urine.
Therefore it’s almost always best to ensure that the body has more calcium than it needs. You want your body to never have cause to take calcium out of the bones.
The most commonly ignored recommendation to prevent osteoporosis is weight-bearing exercises. Walking, hiking, pickleball, dancing, and lifting weights are all weight-bearing exercises. These also count as aerobic exercises.
If you put exercise your heart and exercise your bones on your to-do list, you’ll be able to cross two things off at the same time. In many communities one can find “bone builder” exercise classes which are specifically designed to build bone density.
Some surprising things that can help prevent osteoporosis
The following recommendations are not as well tested as the calcium, vitamin D, and weight-bearing exercise recommendations, but they may help. They are very unlikely to harm most people.
Several small studies done at Penn State show that eating 6 prunes a day for six months can slow the loss of bone in osteopenic women. Prunes do not contain calcium. It is not known what causes the bone protective effect. It is also not known if prune juice conveys the same benefits.
They tested 12 prunes against 6 and 6 was enough to give the benefit and 12 was a little harder to tolerate. If you find the constipating effects of calcium troublesome, prunes might be a good adjunct to them.
A small study on the effects of high-impact jumping on bone strength in pre-menopausal women found a significant improvement in bone density from doing two daily sets of twenty jumps with 30 seconds between each jump.
Don’t try this without consulting with your doctor! High-impact jumping is a terrible idea for some women, especially those who already have osteoporosis, but it can be a good approach for other women.
Osteoporosis prevention is a hard sell because the treatment plan makes the patient feel worse typically. Additionally, if the treatment plan works, the patient doesn’t notice anything.
Not only is it hard to notice and appreciate something not happening, the real misery of osteoporosis seldom sets in until a woman is in her 80’s. It’s difficult to convince a 65 year old woman to do something unpleasant to benefit herself at 85. Many of them tell me, “I won’t live long enough to benefit from that!”.
It is my job to be the adult; and encourage them to take care of themselves as most of them are likely to live into their 80s.
How to know if you have osteoporosis
The test for osteoporosis is a bone-density x-ray. These tests are often done in the same facility that does mammograms, allowing many patients to get back to back appointments.
Because osteoporosis is most common in postmenopausal women, and because it develops slowly, we usually do bone density tests on women when they turn 65. Some experts say if this test shows normal bone density then no further testing is needed. Others say to check again in ten years.
Women with multiple risk factors or women who have had bone fractures from minor injuries should be tested earlier than age 65.
Back to Trudy’s back
I recommended that Trudy take up high-impact jumping and add the prunes, chewable calcium, and vitamin D. If her constipation persists, she will need to figure out a bowel regimen to make the calcium tolerable. This might be as minimal as a small daily glass of prune juice, or it may require laxatives. We talk about investigations to see if she has any additional things causing her bone deterioration and decide that ten further years, a low calcium diet, and a lack of exercise are enough to explain it.
Now that Trudy has osteopenia, her bone density should be tested again in 2 or 3 years to monitor how well her prevention program has been working.
To find out what happens next to Trudy, please click here.
* Since it’s true that if you’re at risk of osteoporosis you should take vitamin D;, I gave this patient the pseudonym of “Trudy.” Trudy is actually an amalgam of several patients. Any resemblance to a specific patient is just a coincidence due to how common osteoporosis is. This article is for the edification of the public. It’s not personal medical advice. Talk to your doctor to get medical advice.
I laughed out loud at "An article about constipation is in the pipeline, but it is taking me a while to get it out."
Great article. I shared it with my wife!
Bones have hormone receptors and the deprivation of estrogen post menopause results in nearly universal loss of bone mineral density in women. I’m currently reading The Menopause Society Guidelines on menopause hormone therapy and planning to break this down in an upcoming post.
I’m angry for Boomer women who were deprived of hormone therapy for 2 decades due to the flawed and overstated data from the Women’s Health Initiative.
“For women aged younger than 60 years or who are within 10 years of menopause onset and have no contraindica-
tions, the benefit-risk ratio is favorable for treatment of bothersome VMS and prevention of bone loss.”
https://menopause.org/wp-content/uploads/professional/nams-2022-hormone-therapy-position-statement.pdf